Medical disclaimer: This article discusses brain death, withdrawal of life support, and organ donation — topics that may be distressing. It is for general health education only and does not replace medical, legal, or pastoral guidance for any individual case. If your family is facing these decisions, ask the treating team to explain findings in plain language and request support from
hospital counselling or chaplaincy services. The Ventilator Is Still Breathing — but the Brain Is Gone. Brain death is not a deep sleep waiting to end. It is death, confirmed by criteria most families have never heard explained.
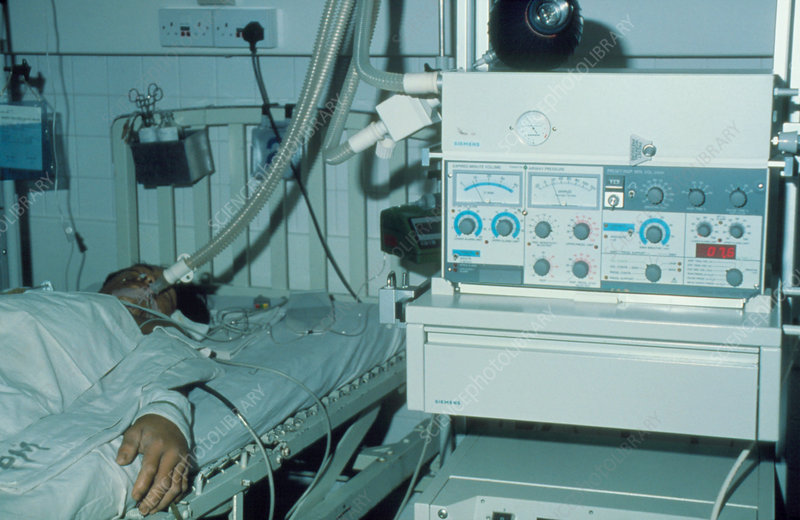
The monitors in a teaching hospital ICU show a steady heartbeat. The ventilator delivers each breath with mechanical precision. To someone walking past the cubicle, the scene can look like sleep — a patient being kept alive until the body mends. But the neurology team has already completed its examination twice. The pupils are fixed and unreactive. Corneal, gag, and cough reflexes are absent. When the head turns, the eyes stay still. Apnoea testing shows no breath when the machine steps back and carbon dioxide rises. An EEG, where available, shows no electrical activity. By accepted medical criteria, this person is dead —
even though the chest still rises and falls.
That gap between what the machines show and what medicine means by death is where confusion, grief, and conflict begin. In Ghana’s major hospitals — and increasingly in regional centres with intensive care — families encounter brain death without ever having heard the term before the worst day of their lives. Understanding it matters for doctors, nurses, and the public alike.

What Brain Death Is — and What It Is Not
Brain death is the irreversible cessation of all functions of the entire brain, including the
brainstem.
That means:
No consciousness
No awareness
No ability to breathe independently
No brainstem reflexes
No possibility of recovery
Even when machines maintain circulation and oxygenation, the individual is medically and legally dead once brain death is confirmed according to accepted standards. The ventilator is not healing a sleeping brain. It is temporarily perfusing organs after neurological death has occurred.
Brain death is not coma. It is not vegetative state.
Condition Brain activity Brainstem
reflexes
Breathing Recovery possible?
Coma Reduced Usually present May be present Yes
Vegetative state Partial Present Present Sometimes
Brain death Absent Absent Absent No
A patient in coma may still have brain activity and a path toward recovery. In vegetative state, brainstem function persists. In brain death, the entire brain including the brainstem has permanently ceased functioning. There is no documented recovery after properly confirmed brain death.The brainstem controls breathing, heart rate regulation, consciousness pathways, swallowing, and pupillary responses. Loss of brainstem function means the body cannot sustain life independently — regardless of what the ECG trace suggests.
How Catastrophic Brain Injury Becomes Irreversible Death
Brain death develops through a sequence many ICU staff recognise but families rarely see described.
SIRBL maps the pathophysiology:
Severe injury — bleeding, swelling, oxygen deprivation, trauma
Increased intracranial pressure — the rigid skull allows nowhere for swollen tissue to go
Reduced blood flow — when intracranial pressure exceeds arterial pressure, blood cannot
enter the brain
Brain herniation — swollen tissue shifts and compresses the brainstem
Loss of brainstem function — respiratory drive, reflexes, and consciousness pathways fail
Neurons die permanently from lack of oxygen and circulation. At that stage, recovery is
impossible — not unlikely, impossible.
Causes
Brain death results from catastrophic, irreversible brain injury. Common causes include:
Severe traumatic brain injury — road traffic accidents, gunshot wounds, falls, assault; massive trauma causes swelling and bleeding that destroy tissue
Stroke — large hemorrhagic or ischemic strokes raising intracranial pressure and stopping cerebral blood flow
Hypoxic-ischaemic brain injury — cardiac arrest, near drowning, severe respiratory failure, suffocation
Intracranial haemorrhage — subarachnoid or intracerebral bleeding compressing structures
Brain tumours — large or rapidly expanding masses compressing the brainstem
Severe infections — meningitis and encephalitis producing massive swelling
Drug overdose and toxic injury — prolonged oxygen deprivation leading to irreversible damage
Some clinicians recall SHIT–B: Stroke, Hypoxia, Infection, Trauma, Bleeding. Risk factors include uncontrolled hypertension, cardiovascular disease, substance abuse, advanced age, and poorly controlled diabetes. Road traffic crashes and cardiac arrest resuscitated at a district hospitalmay end, after transfer to a teaching hospital ICU, in the solemn work of confirming brain death.
What Brain Death Looks Like at the Bedside
Brain death produces complete absence of neurological function — with one importantexception.
NO BRAIN captures the clinical picture:
No response — no consciousness, no purposeful movement, no reaction to pain
Oxygen drive absent — apnoea; breathing occurs only through mechanical ventilation
Brainstem reflexes absent — pupils fixed, no corneal blink, no gag or cough
Reflexes absent — oculocephalic and oculovestibular reflexes show no eye movement
Apnoea confirmed on formal testing
Irreversible — known cause, confounders excluded
No recovery possibleMuscle tone is flaccid.
Spontaneous voluntary movement does not occur.
Spinal reflexes can mislead. Some spinal reflexes may persist after brain death — finger jerks, toe movement, spinal automatisms. These do not indicate brain function. Families sometimes seize on a twitch as hope. Clinicians must explain gently that spinal cord reflexes are not consciousness returning.
How Brain Death Is Diagnosed — and What Must Be Ruled Out First
Diagnosis follows strict protocols. Requirements for number of examiners, observation periods, ancillary testing, and consent vary by country — Ghana’s legal framework continues to evolve — but core principles are shared in teaching hospitals worldwide.
Before testing begins .
Doctors must establish:
- Known cause of brain injury capable of causing irreversible damage
- Irreversibility of the condition
- Exclusion of confounding factors that mimic brain death
- Confounders that must be corrected first include hypothermia, drug intoxication, sedative medications, severe metabolic disturbances, and neuromuscular blockade. A phrase taught in critical care captures the hypothermia rule: “You are not dead until warm and dead.” Low body temperature can suppress reflexes and mimic death.
Conditions that mimic brain death also include locked-in syndrome — where patients are conscious but unable to move — and severe metabolic disorders such as hypoglycaemia or hepatic encephalopathy.
Core clinical criteria
Diagnosis rests on three pillars — CAP:
Coma — deeply unconscious and unresponsive
Apnoea — no spontaneous breathing when tested
Pupils and brainstem reflexes absent — all brainstem reflexes must be absent
Apnoea testing
The patient is preoxygenated. Ventilator support is temporarily reduced. Carbon dioxide is allowed to rise. If no respiratory effort occurs despite elevated carbon dioxide, the test supports brain death — confirming that the brainstem respiratory drive is gone.
Ancillary tests when needed
When clinical testing cannot be completed or doubt remains, additional tests may include:
Electroencephalography (EEG) — absence of electrical brain activity
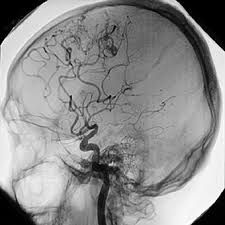
Cerebral angiography — absence of cerebral blood flow
Nuclear medicine brain scan — lack of perfusion
Transcranial Doppler ultrasound — absent cerebral circulation
At regional hospitals without ancillary capacity, referral or repeat examination by experienced intensivists may be necessary — accuracy matters more than speed.
Why Life Support Comes Off After Confirmation
Even while the ventilator runs, organ systems begin failing after brain death: blood pressure becomes unstable, hormonal control collapses causing diabetes insipidus and electrolyte disturbance, temperature regulation fails, and infection risk rises. Eventually heart, kidneys, and liver fail. The machine postpones collapse — for family processing and, when consent exists, organ procurement — but does not reverse death. Life support includes mechanical ventilation, vasopressors, artificial nutrition, and dialysis.
After confirmed brain death, continuing invasive treatment offers no curative benefit because the patient is already dead. Machines maintain circulation temporarily; they do not restore a living brain. There is no documented recovery after proper confirmation.
Removal follows medical, ethical, and legal reasoning: autonomy (honouring known wishes), beneficence, non-maleficence, and justice in using ICU beds and ventilators Ghana’s health system cannot spare indefinitely. Prolonged maintenance can deepen family distress by sustaining false hope.
Speaking with Families — and What the Public Gets Wrong
Doctors should communicate compassionately and clearly. Families often need time to absorb information that contradicts what their eyes see. Essential messages:
Brain death is irreversible
The ventilator maintains organ function artificially — it is not a sign of recovery ahead
The person they knew cannot return
Brain-dead patients do not feel pain; consciousness and sensation are absent
Misconceptions persist:
“It is just a coma.” False. Coma may improve; brain death cannot.
“The patient might feel the withdrawal.” False. Without brain function, there is no perception.
“The machine is keeping them alive.” Partially true in appearance only. Circulation continues temporarily after death is established; the machine is not restoring a living brain. Grief counselling and chaplaincy support help families and staff. Brain death affects communities, not only ICUs.

Organ Donation, Law, and Ghanaian Realities
Brain death enables organ transplantation — heart, kidneys, liver, lungs, and pancreas from one donor may save several lives. Public education improves acceptance; mistrust grows when families believe death is declared prematurely to harvest organs. Transparent criteria, independent confirmation where required, and compassionate timing build trust.
Ghana continues developing legal frameworks for brain death determination and transplantation centred at teaching hospitals. District hospitals stabilise and transfer; confirmation typically occurs at tertiary ICU level. Irreversible loss of all brain function,
including the brainstem, is death — even when the monitor still beeps. Families navigating NHIS and out-of-pocket ICU costs need social work support alongside medical honesty.
What to Carry Forward
For clinicians: apply criteria rigorously, exclude confounders, document clearly, explain in plain language. For nurses: reinforce the team’s message with consistency and kindness. For the public: the rising chest is not proof of a living mind. When brain death is confirmed, stopping life support is not abandonment — the person has died, and the machine was always going to stop. What remains is dignity for the deceased, honesty for the living, and — when chosen — organs that let others breathe again. In Ghana’s
hospitals, where families meet this without warning, how we explain it may matter as much as how we diagnose it.
Disclaimer
The information contained in this post is for general information purposes only. The information is provided by When To Pronounce A Patient Brain Dead and while we endeavour to keep the information up to date and correct, we make no representations or warranties of any kind, express or implied, about the completeness, accuracy, reliability, suitability or availability with respect to the website or the information, products, services, or related graphics contained on the post for any purpose.