Medical disclaimer: This article is for general health education only. It does not replace examination, diagnosis, or treatment by a qualified doctor. Persistent hip, groin, knee, or shoulder pain — especially if you use steroids, have sickle cell disease, or have had a hip injury — should be evaluated at a health facility. Do not stop prescribed medications without medical advice.
Hip Pain in Someone on Steroids Is Not Always Ordinary Arthritis. Avascular necrosis can stay silent until the bone collapses and by then the window has narrowed.
A man in his late thirties sits on an examination couch at a district hospital in Kumasi. He has been on prednisolone for months -treatment for an autoimmune condition managed at a regional centre. His complaint sounds ordinary: aching in the groin, stiffness when he rises from a chair, a slight limp that his family noticed before he did.The medical officer checks for infection, considers ordinary wear-and-tear, and orders an X-ray. The film looks nearly normal. He is sent home with pain tablets and advice to rest.
Six months later, at a teaching hospital orthopaedic clinic, an MRI tells a different story. The femoral head shows early avascular necrosis — bone dying from lack of blood supply, damage already advanced enough that simple rest will not reverse it. That sequence is not rare. It is, in many ways, the story of avascular necrosis.
What Avascular Necrosis Actually Is
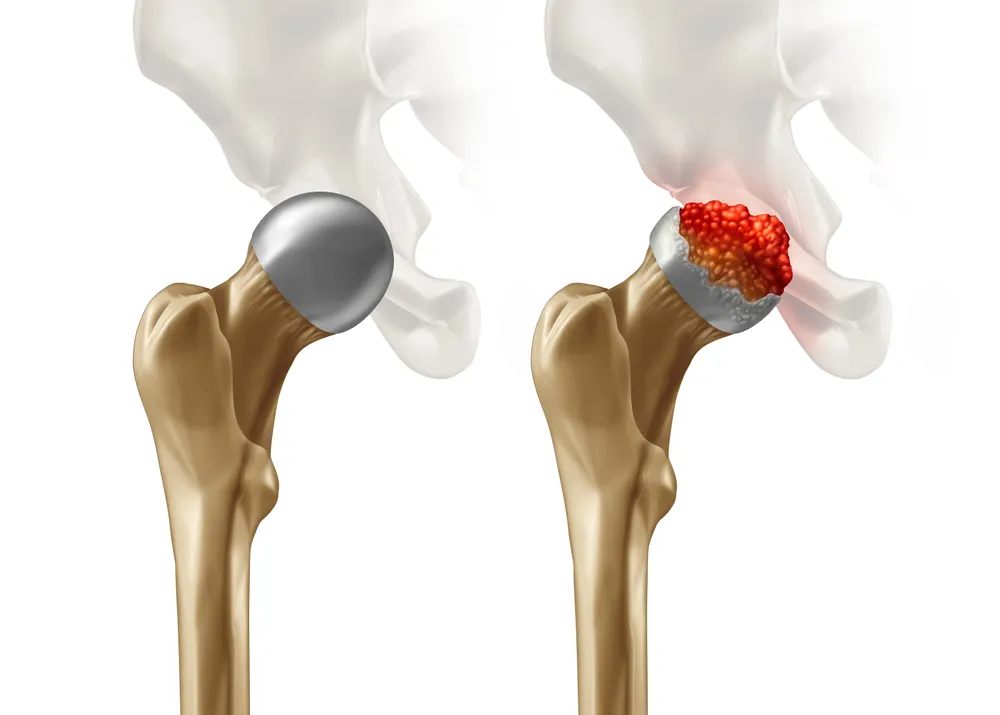
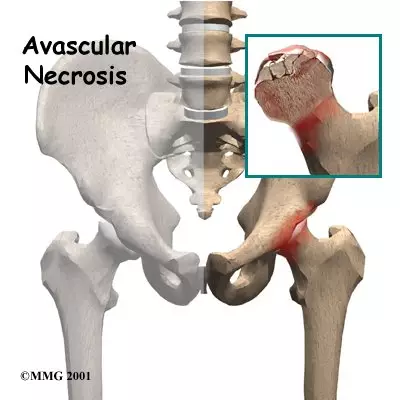
Avascular necrosis — also called osteonecrosis, ischemic bone necrosis, or bone infarction — is the death of bone tissue caused by inadequate blood supply. Bone cells depend on constant circulation for oxygen and nutrients. When blood flow is reduced or interrupted, osteocytes die, bone structure weakens, microfractures develop under everyday stress, and the affected surface may eventually collapse. Secondary arthritis often follows.The disease can affect one bone or several at once. Although any bone can be involved, the hip joint — particularly the femoral head — is the most common site. Shoulders, knees, ankles,
and wrists are also affected; in the wrist, the scaphoid and lunate are especially vulnerable.
Avascular necrosis commonly affects adults between 30 and 50 years of age. Men are slightly more affected than women. If not diagnosed and treated early, it leads to severe pain, joint destruction, disability, and lasting arthritis. Early stages may show few or no symptoms — which is precisely why diagnosis is often delayed until significant damage has already occurred.
Causes: Trauma, Steroids, and Everything in Between Blood flow to bone fails for many reasons. Causes divide broadly into traumatic and non- traumatic.
Traumatic causes
Direct injury to vessels supplying bone is the mechanism:
Fractures, especially of the femoral neck
Joint dislocation, particularly hip dislocation interrupting femoral head circulation
Severe crushing trauma damaging surrounding vessels
Road traffic injuries seen at Ghana’s emergency departments make traumatic avascular necrosis a real consideration after hip and femoral neck fractures — not only months later when pain persists, but at initial follow-up.
Non-traumatic causes
These matter enormously in outpatient practice. Clinicians sometimes use STARRS to recall the major non-traumatic contributors:
Steroids — long-term corticosteroid therapy is one of the most common causes
Trauma — overlapping category, but worth separating in history-taking
Alcohol — chronic heavy use damages vessels and fat metabolism
Radiation — radiation therapy can impair bone circulation
Rheumatologic disease — autoimmune conditions such as systemic lupus erythematosus, often compounded by steroid treatment
Sickle cell disease — sickled cells block small vessels supplying bone
Other causes include decompression sickness, organ transplantation with high-dose steroids, blood clotting disorders, hyperlipidemia, and idiopathic cases where no trigger is found. Prolonged prednisolone or dexamethasone may increase fat deposition, compress vessels, and reduce bone circulation — risk rises with high doses and long duration. Hip pain in a steroid user should raise immediate suspicion for avascular necrosis, especially where district-level follow-up is limited. The same applies to anyone with sickle cell disease: femoral head necrosis belongs on the differential for hip pain, not only after an obvious vaso-occlusive crisis.

How the Bone Dies: From Blocked Flow to Collapse
Pathophysiology progresses in stages that explain both the silent early phase and the dramatic
late one:
- Reduced blood supply — from vessel injury, clot, fat emboli, or compression
- Bone cell death — osteocytes and marrow cells die without oxygen
- Structural weakening — dead bone loses strength
- Microfractures — tiny fractures under normal load
- Bone collapse — in the hip, the femoral head flattens
- Secondary arthritis — cartilage degenerates; osteoarthritis develops
The mnemonic BLOCK walks the same path: Blood supply loss, Loss of bone cells, Osteocyte death, Collapse of bone, Knee/hip arthritis. Symptoms often appear only after significant bone damage — the central tragedy of this
disease.
Stages and What Patients Feel
Disease stage shapes both symptoms and imaging.
Stage Features
Stage 1 Early disease; X-rays may appear normal; MRI detects abnormality
Stage 2 Bone changes visible on X-ray; no collapse yet
Stage 3 Collapse begins; crescent sign may appear
Stage 4 Severe collapse; arthritis develops
Symptoms depend on bone affected, stage, and severity. Early disease may be silent. When pain arrives, it is usually deep, throbbing, and gradually worsening. In hip avascular necrosis, pain localises to the groin, buttock, or thigh — sometimes referred to the knee. Knee involvement worsens with walking or standing. Shoulder disease limits arm movement. Stiffness and reduced range of motion follow. Limping appears, especially in hip disease. Advanced stages bring difficulty bearing weight, joint deformity, and severe disability.
PLAIN summarises the symptom cluster many patients eventually report: Pain, Limping, Arthritis
later, Immobility, Necrosis of bone. Do not wait for all five before investigating a high-risk patient with groin pain.
Diagnosis: History First, MRI When X-Ray Lies Early diagnosis is extremely important because treatment before collapse offers the best chance of preserving the joint. Delayed diagnosis worsens outcomes — full stop.
History
Ask directly about steroid use — dose and duration. Ask about alcohol. Ask about trauma, fractures, and dislocations. Ask about sickle cell status, autoimmune disease, radiation, and transplant history.
Examination
Painful joint movement, limping, and reduced mobility may be present even when X-rays look
deceptively normal. Imaging X-ray is useful in later stages, showing bone collapse, joint narrowing, or the crescent sign. A
normal X-ray does not exclude early disease. MRI is the most sensitive test and can detect avascular necrosis before X-ray changes appear.
When suspicion is high and X-ray is normal — as in the Kumasi patient above — MRI is the investigation that changes management. Referral from district hospital to a centre with MRI capacity is often the decisive step. CT scan shows detailed bone structure. Bone scan may identify reduced blood flow.
Laboratory tests
Labs mainly uncover underlying causes: lipid profile, autoimmune markers, sickle cell testing, and other directed studies — not to diagnose necrosis directly, but to explain it and guide prevention elsewhere in the body.
Differential diagnosis
Conditions that mimic avascular necrosis include osteoarthritis, fractures, septic arthritis, bone tumours, and rheumatoid arthritis. Red flags for infection — fever, hot joint, systemic illness — must not be missed in the rush toward an orthopaedic diagnosis.
Complications When Treatment Comes Late
Without treatment, avascular necrosis progresses predictably. PAINS captures the toll:
Pain — chronic and severe
Arthritis — secondary osteoarthritis after collapse
Immobility — walking and daily activities become difficult
Necrotic collapse — major structural failure
Structural deformity — altered joint anatomy
Chronic pain and disability also affect employment, relationships, and mental health — supportive care and rehabilitation matter alongside surgery.
Management: Preserve the Joint If You Can, Replace It If You Must
Treatment depends on disease stage, bone involved, and severity. Early treatment aims to preserve the joint.
Non-surgical management
Activity modification — reducing weight-bearing with crutches or limited walking slows progression
Pain control — NSAIDs and other analgesics as appropriate
Physiotherapy — maintains mobility and muscle strength
Treating underlying causes — controlling sickle cell disease, reducing alcohol, adjusting steroid therapy only under specialist nsupervision
Bisphosphonates — may slow bone destruction in some cases At district level, what is often achievable immediately is recognising the problem, limiting weight-bearing, controlling pain, and referring early to orthopaedic or rheumatology services- before collapse makes joint preservation impossible.
Surgical management
Surgery becomes necessary as disease advances:
Core decompression — drilling into bone to reduce pressure and improve blood flow; most useful in early stages
Bone grafting — replacing damaged areas with healthy bone tissue
Osteotomy — repositioning bone to reduce stress on the affected segment
Joint replacement — when destruction is severe; total hip replacement is common after advanced femoral head collapse and can restore mobility and reduce pain. Rehabilitation after any intervention focuses on movement, strength, and preventing stiffness.
Prevention and Referral in Ghana
Some cases cannot be prevented, but risk can be lowered: lowest effective steroid dose, limited alcohol, smoking cessation, prompt fracture care, and control of sickle cell disease, autoimmune disorders, and hyperlipidemia. Prescribers should warn steroid patients to report new groin or hip pain early. CHPS workers and district hospitals can capture history and begin evaluation; MRI and surgery concentrate at regional and teaching hospitals. NHIS covers many consultations, but MRI, core decompression, and joint replacement still mean waiting lists and travel from rural districts. Early referral beats late heroic surgery — biology does not wait for logistics.
What to Remember
Avascular necrosis is bone death from lost blood supply, most often in the hip of adults aged 30 to 50. It stays quiet while the bone weakens. X-rays lie early; MRI tells the truth sooner. Treatment before collapse preserves joints; after collapse, replacement often becomes the only option. If you have groin pain and a steroid packet in your bag, do not accept “probably arthritis” without proper evaluation. If you prescribed the steroids, treat hip pain as avascular necrosis until proven otherwise. The minor limp today may be the collapse that limits walking tomorrow.
Disclaimer
The information contained in this post is for general information purposes only. The information is provided by Avascular Necrosis And It's Complication and while we endeavour to keep the information up to date and correct, we make no representations or warranties of any kind, express or implied, about the completeness, accuracy, reliability, suitability or availability with respect to the website or the information, products, services, or related graphics contained on the post for any purpose.