Medical disclaimer: This article is for general health education only. It does not replace
examination, diagnosis, or treatment by a qualified doctor. If you notice persistent changes in
your hands, feet, face, or vision, please seek care at your nearest health facility.
Acromegaly Is Easy to Miss — Until the Hands No Longer Fit. The ring gets tight. The shoes go up a size. Years pass before anyone connects it.
A woman in her early forties walks into a clinic in Kumasi complaining of joint pain and tiredness. Her blood pressure is high. She sweats more than she used to. The nurse notes her ring feels tight, but nobody thinks much of it — she has gained weight, after all, and life is stressful. Two years later, at a teaching hospital, someone finally asks to see an old photograph. The jaw
looks different. The nose is broader. The hands are unmistakably larger. An IGF-1 test comes back elevated. An MRI shows a pituitary adenoma. That delay is not unusual. It is, in many ways, the story of acromegaly.
What Acromegaly Actually Is
Acromegaly is a hormonal disorder caused by too much growth hormone (GH) in adulthood — after the growth plates in your bones have already closed. Instead of making you taller, the excess hormone thickens and enlarges bones, soft tissues, and internal organs over months and years.
The usual chain looks like this: a pituitary tumour (most often a benign adenoma) secretes excess GH. The liver responds by producing too much insulin-like growth factor-1 (IGF-1). IGF-1 is what drives the visible and internal changes — enlarged hands and feet, coarse facial features, organ enlargement, joint damage, and metabolic problems. It is uncommon, but clinically important. Men and women are affected equally, typically between ages 30 and 50. Because the changes happen slowly, diagnosis is often delayed by several years — sometimes five to ten — even in well-resourced health systems. In settings where endocrine specialists and pituitary imaging are concentrated in major centres, that delay can stretch longer still.
Acromegaly vs Gigantism
Both conditions involve excess growth hormone. The difference is timing: Condition When it starts Main effect
Gigantism Before growth plates close
In Gigantism growth plates close before childhood resulting in excess height where as in acromegaly growth plates close after (adulthood) with Enlarged body parts, not height
If you are seeing a child who is growing abnormally tall with hormonal signs, think gigantism. If you are seeing an adult whose features and extremities are changing, think acromegaly.
Why It Gets Overlooked
Here is the reframe that matters for both clinicians and patients: acromegaly is rarely dramatic at first. People adapt. They buy bigger shoes. They stop wearing rings. They attribute joint pain to age or hard work. Family members may not notice gradual facial change.Many patients only realise something is wrong when they compare a current photo to one from five years ago.
That means the barrier to diagnosis is not usually patient denial. It is the nature of the disease —slow, insidious, and easy to scatter across separate complaints handled at different visits.
Hypertension at one clinic. Snoring at another. Carpal tunnel symptoms somewhere else. Each gets treated in isolation while the underlying cause goes unrecognised. For health workers in Ghana — whether you practise at a CHPS compound, a district hospital, a polyclinic, or a tertiary centre — the practical lesson is simple: when the pattern does not fit ordinary ageing or isolated diagnoses, widen the lens.
Causes and Who Is at Risk
Pituitary adenoma (most common)
Roughly nine out of ten cases come from a benign tumour in the pituitary gland producing excess GH. Tumours may be:
Microadenomas — smaller than 10 mm
Macroadenomas — 10 mm or larger; these may compress nearby structures, including the optic chiasm
Ectopic GH secretion (rare)
Occasionally, tumours outside the pituitary — in the lungs or pancreas, for example — produce
GH or growth hormone-releasing hormone (GHRH).
Genetic syndromes (rare)
Conditions such as multiple endocrine neoplasia type 1 (MEN1) and McCune-Albright syndrome can increase risk. A family history of endocrine tumours should raise your index of suspicion. There are no clear lifestyle risk factors — this is not a disease you prevent by diet or exercise alone. What you can do is recognise it early.
How the Disease Progresses
A useful way to think about pathophysiology:
- Excess GH — usually from a pituitary adenoma
- Raised IGF-1 — the liver’s response to sustained GH stimulation
- Tissue overgrowth — bones, cartilage, soft tissues, and organs enlarge
- Organ involvement — heart, liver, thyroid, and other organs may be affected
- Metabolic effects — insulin resistance, impaired glucose tolerance, hypertension
- Mass effect — large tumours compress the optic chiasm and surrounding structures
Clinicians sometimes use the mnemonic GROWS: Growth hormone excess, Raised IGF-1, Organ enlargement, Widened bones, Soft tissue overgrowth.
What to Look For: Signs and Symptoms
Symptoms develop gradually. Listen for clusters, not single complaints.
The classic clues
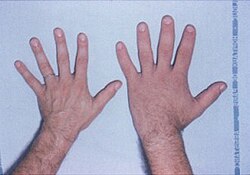
Enlarged hands and feet — increased shoe size, tight rings, gloves that no longer fit
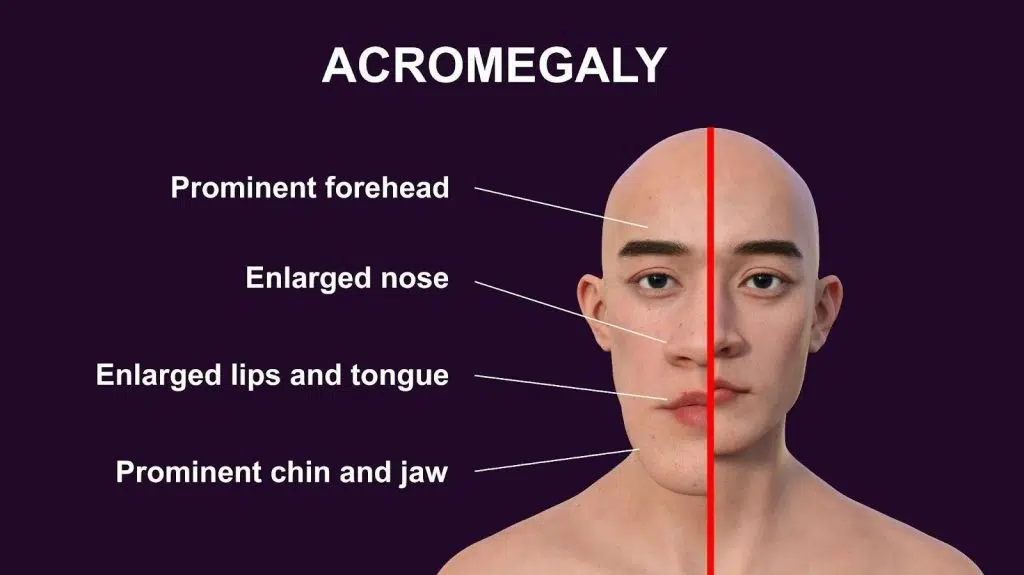
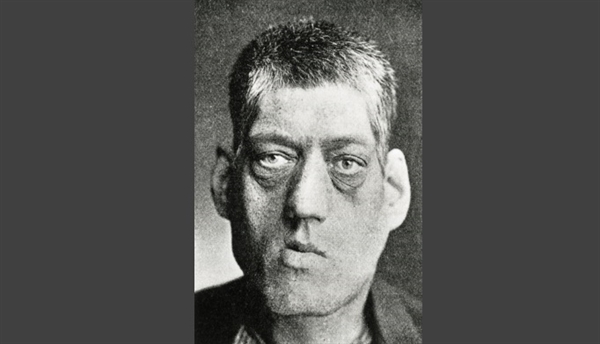
Coarse facial features — enlarged nose, thick lips, prominent jaw, broad forehead
Prognathism — forward protrusion of the lower jaw
Macroglossia — enlarged tongue; may affect speech, breathing, and sleep
Thickened, oily, sweaty skin
Excessive sweating — very common and often underappreciated
Other important features
Joint pain and arthritis-like symptoms from cartilage damage
Headache from tumour pressure
Visual problems — blurred vision or loss of peripheral vision (bitemporal hemianopia) when the optic chiasm is compressed
Fatigue and weakness
Carpal tunnel syndrome — numbness, tingling, hand weakness
Deepened voice from soft tissue thickening
Obstructive sleep apnoea from airway narrowing
Menstrual irregularities or infertility in women; erectile dysfunction in men
Hypertension
Type 2 diabetes from GH-induced insulin resistance
Another mnemonic some clinicians use: ACROMEGALY — Arthritis, Coarse features, Ring size increase, Organ enlargement, Macroglossia, Excess sweating, Glucose intolerance, Apnoea, Large hands/feet, Years of slow progression. That last letter is the one worth remembering in busy outpatient departments: years.
Diagnosis: What to Order and When to Refer
Diagnosis rests on clinical suspicion confirmed by hormonal testing and imaging.
Start with the history
Ask directly about shoe and ring size. Ask about facial changes — and look at old photographs if the patient has them. Ask about headaches, vision changes, snoring, and sweating.
Physical examination
Look for enlarged extremities, coarse facial appearance, skin thickening, prognathism, macroglossia, and hypertension.
Key investigations
Test Role
Serum IGF-1 Best screening test; elevated levels support the diagnosis
Oral glucose suppression test In acromegaly, GH stays elevated despite glucose load; normally GH should suppress
Pituitary MRI Identifies adenoma; the most important imaging study
Visual field testing Assesses optic chiasm compression
Depending on complications, you may also need blood glucose, echocardiography, sleep studies, and colonoscopy — acromegaly carries increased risk of colon polyps and colorectal cancer. A note for practice in Ghana IGF-1 testing and pituitary MRI may not be available at every facility. If your clinical suspicion is high — especially with enlarged extremities, progressive facial change, diabetes and hypertension together, or visual symptoms — refer early to a centre with endocrine and radiology capacity. Teaching hospitals in Accra, Kumasi, Tamale, and other regional hubs are often where the diagnostic pathway completes. Do not wait for every symptom to align perfectly. Partial pictures are common.
Complications If Treatment Is Delayed
Untreated acromegaly affects the whole body. Major complications include:
Cardiovascular disease — hypertension, cardiomyopathy, heart failure; a leading cause of mortality
Diabetes mellitus from insulin resistance
Obstructive sleep apnoea
Arthritis and chronic joint pain
Colon polyps and increased colon cancer risk
Vision loss from optic pathway compression
Hypopituitarism when the tumour compresses normal pituitary tissue
Nerve compression syndromes such as carpal tunnel
Anxiety, depression, and social distress from visible physical change
Reduced life expectancy when the disease remains uncontrolled
The mnemonic HARD CAPS captures much of this: Heart disease, Arthritis, Respiratory (sleep) apnoea, Diabetes, Colon polyps, Anxiety/depression, Pituitary failure, Sight problems.
Conditions That Can Look Similar
Before confirming acromegaly, consider:
Hypothyroidism (coarse features, but different hormonal profile)
Paget disease of bone
Familial coarse facial features
Gigantism (if the patient is still growing)
Treatment: What Success Looks Like
Treatment aims to normalise GH and IGF-1 levels, shrink or remove the tumour, relieve symptoms, and prevent complications.
Surgery — first line for many patients Transsphenoidal surgery — removing the tumour through the nasal cavity — is often the first- line treatment, especially for smaller adenomas. Outcomes are best when the tumour is micro-or macroadenoma with favourable anatomy and an experienced surgical team.
Medical therapy
When surgery is incomplete or not suitable:
Somatostatin analogues (octreotide, lanreotide) — reduce GH secretion
Dopamine agonists (cabergoline) — may help in some cases
GH receptor antagonists (pegvisomant) — block GH action at the receptor
Radiation therapy
Considered when surgery and medication do not achieve control. Effects may take years; long- term follow-up is essential.
Managing complications
Treat diabetes, hypertension, sleep apnoea, and arthritis alongside the primary disease. Lifestyle support — healthy diet, regular exercise, psychological counselling — matters. Many patients struggle emotionally for years before anyone names the condition. Validation helps.
Prognosis: Early Is Everything
Prognosis depends on tumour size, how completely treatment controls hormone levels, and whether complications have already developed. The encouraging truth: early diagnosis and proper treatment can significantly improve symptoms, quality of life, and survival. Many patients treated successfully can expect a normal life expectancy. The opposite is also true. Years of uncontrolled GH excess leave damage that cannot always be fully reversed — which is why the photograph comparison and the tight ring matter more than they seem.
What Patients and Families Should Know
If you are reading this because something about your body — or someone you love — has been changing slowly, you are not being vain for noticing. You are not “just getting older” if your shoe size has gone up twice in five years and your face looks different in every mirror but your own memory. Bring old photos to your appointment. Tell your doctor about the ring that no longer fits. Ask about IGF-1 if facial and hand changes are progressing together. Ask for referral if you are not
being heard. If you are a clinician who sees one patient like this a year, that patient is counting on you to remember that acromegaly exists — even when the lab results are still pending.
Key Takeaways
Acromegaly is excess growth hormone in adulthood, most often from a pituitary adenoma
Changes are slow; diagnosis is commonly delayed for years
Enlarged hands and feet, coarse facial features, sweating, joint pain, and metabolic disease should trigger suspicion
IGF-1 is the best screening test; MRI confirms the tumour
Treatment combines surgery, medication, and complication management
Early referral and early treatment change outcomes dramatically
Success in acromegaly is often partial at first — a controlled IGF-1, a preserved visual field, a patient who finally understands what has been happening to their body. That partial success is worth pursuing from the first visit where the pieces start to fit.
For specialist endocrine care in Ghana, ask your primary clinician about referral to a teaching hospital or accredited endocrine service. If you are a health worker and want to discuss a suspected case, document the clinical pattern, request IGF-1 where available, and refer without delay when suspicion is high.
Disclaimer
The information contained in this post is for general information purposes only. The information is provided by Overview of Acromegaly And Gigantism and while we endeavour to keep the information up to date and correct, we make no representations or warranties of any kind, express or implied, about the completeness, accuracy, reliability, suitability or availability with respect to the website or the information, products, services, or related graphics contained on the post for any purpose.



