Medical disclaimer: This article is for general health education only. It does not replace
examination, diagnosis, or treatment by a qualified doctor. Diabetic ketoacidosis and
hyperosmolar hyperglycemic state are medical emergencies. If you or someone you know has
severe thirst, confusion, vomiting, or difficulty breathing with known or suspected diabetes, go
to the nearest health facility immediately.

A teenager arrives at an emergency unit in Accra brought in by a worried aunt. He has been urinating constantly for two days, drinking water by the bucket, and vomiting since morning. He looks thin, his lips are dry, and he is breathing as if he has just run a race — fast and deep. When the nurse leans close, there is a faint fruity smell on his breath. His aunt says he was diagnosed with type 1 diabetes last year but has been “doing fine” and sometimes skips insulin when money is tight or he feels well. Nobody thought to increase his doses when he developed a cough three days ago. That presentation — rapid, dangerous, and often preventable — is diabetic ketoacidosis. And in Ghana, where type 1 diabetes in children and young adults still too often presents as a first-time emergency rather than a managed chronic illness, DKA remains a condition every clinician, nurse, and family member needs to recognise early.
Two Emergencies, One Disease
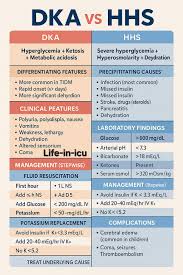
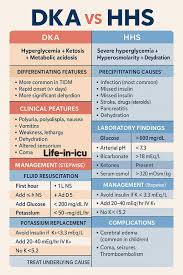
Diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS) are both life- threatening complications of diabetes mellitus. Both result from severe disturbances in insulin activity and blood glucose regulation. Both can progress rapidly to shock, coma, organ failure, and death without proper management. The difference matters at the bedside. DKA is an acute metabolic complication characterised by severe hyperglycemia, ketone production, metabolic acidosis, and dehydration. It develops because the body lacks enough insulin to use glucose for energy, forcing fat breakdown instead. That fat metabolism produces
acidic compounds called ketones — acetoacetate and beta-hydroxybutyrate.
HHS is characterised by extreme hyperglycemia, severe dehydration, and high serum osmolality, with minimal or absent ketosis. Enough insulin is usually present to prevent significant ketone formation, but not enough to control blood sugar. Feature DKA HHS
Common diabetes type Type 1 Type 2
Typical age Younger — children, adolescents, young adults
Older — often above 50
Onset Rapid (hours to days) Gradual (days to weeks)
Ketosis Severe Minimal or absent
Acidosis Present Mild or absent
Blood glucose Moderate to high (usually >250 mg/dL)
Extremely high (often >600
mg/dL)
Dehydration Moderate Severe — more profound than DKA
Neurological symptoms Mild to moderate Often severe
The shorthand that saves lives: DKA = severe ketosis and acidosis. HHS = severe dehydration
and hyperosmolarity. Clinicians sometimes use KAD for DKA — Ketosis, Acidosis, Dehydration — and HOT for HHS —
Hyperosmolarity, Older patients, Tremendous dehydration.
Who Gets Which Condition
DKA commonly affects children, adolescents, young adults, and patients with type 1 diabetes. Adults with type 2 diabetes can also develop DKA during severe illness. In Ghanaian practice, the young type 1 patient who presents acutely — sometimes before diabetes is ever diagnosed — is the face of DKA I see most often in teaching hospital records and district referrals. HHS usually affects older adults above 50, particularly those with type 2 diabetes. Mortality in HHS is generally higher than in DKA because affected patients are often older with multiple medical conditions.
What Triggers These Crises
Both conditions are usually triggered by stress or insulin deficiency. The most common trigger for both is infection — pneumonia, urinary tract infection, sepsis — because infections increase stress hormones that raise blood glucose. Other common causes include:
Missed insulin or poor medication compliance — never assume this is only patient fault;cost, access, and lack of sick-day education all play a role
Newly diagnosed diabetes — some patients first present with DKA before anyone knows they have diabetes
Myocardial infarction and stroke — both increase stress hormone release
Surgery or trauma — major stress increases insulin requirements
Certain medications — corticosteroids, diuretics, antipsychotics
Substance abuse — alcohol and illicit drugs may contribute
Risk factors for DKA include type 1 diabetes, poor insulin adherence, infection, and psychological stress, most commonly in children, teenagers, and young adults under 40.
Risk factors for HHS include type 2 diabetes, dehydration, dementia, poor fluid intake, and chronic illness — more common in adults above 50 and elderly patients.
How the Body Breaks Down: Pathophysiology
DKA — the KETO pathway
Understanding the cascade helps you treat in the right order:
- Severe insulin deficiency — glucose cannot enter cells effectively
- Counter-regulatory hormones rise — glucagon, cortisol, and adrenaline increase blood
glucose production - Hyperglycemia develops — blood glucose rises significantly
- Fat breakdown occurs — cells cannot use glucose, so the body metabolises fat for energy
- Ketone formation — fat metabolism produces ketones
- Metabolic acidosis — ketones are acidic; blood pH falls
- Osmotic diuresis — high glucose pulls water into urine, causing severe dehydration and
electrolyte loss The mnemonic KETO captures this: Ketone formation, Electrolyte loss, Total insulin deficiency, Osmotic diuresis. HHS — dehydration without ketosis - HHS differs because ketosis stays minimal:
- Relative insulin deficiency — enough insulin exists to suppress fat breakdown
- Extreme hyperglycemia — blood glucose becomes extremely high
- Severe osmotic diuresis — massive fluid loss through urine
- Profound dehydration — patients become severely dehydrated
- Hyperosmolarity — blood becomes highly concentrated, affecting brain function
HHS often presents with more severe neurological impairment than DKA. That is not a subtle point — it changes how urgently you act.
What to Look For
DKA — rapid deterioration
Symptoms usually develop over hours to days:
Polyuria and polydipsia — frequent urination and excessive thirst from osmotic diuresis and dehydration
Weight loss — from fluid and fat loss
Weakness and fatigue — dehydration and electrolyte imbalance
Nausea and vomiting — ketosis irritates the gastrointestinal tract
Abdominal pain — especially common in children; do not dismiss it as unrelated
Fruity breath odour — caused by acetone
Kussmaul breathing — deep, rapid breathing compensating for acidosis
Altered mental status — from confusion to coma
Signs of dehydration — dry mouth, sunken eyes, hypotension, tachycardia
HHS — gradual collapse
Symptoms often develop over days to weeks:
Severe dehydration — more profound than in DKA
Extreme weakness — patients may become severely debilitated
Polyuria and polydipsia — common early symptoms
Neurological symptoms — confusion, hallucinations, seizures, coma; typically more severe
than in DKA
Dry skin and mucous membranes
Hypotension and tachycardia from dehydration
Diagnosis: Clinical Suspicion Plus Labs
Diagnosis rests on clinical findings confirmed by laboratory investigations.
Investigation DKA HHS
Blood glucose Elevated (usually >250 mg/dL)
Elevated (often >600 mg/dL)
Serum ketones Elevated Minimal or absent
Arterial blood gas Metabolic acidosis Mild or no acidosis
Serum bicarbonate Reduced Less affected
Serum osmolality Elevated Markedly elevated
Electrolytes Potassium and sodium
disturbances
Potassium and sodium disturbances
Kidney function May show dehydration- related injury
May show dehydration- related injury
Complete blood count May indicate infection May indicate infection
ECG Assesses potassium-related
cardiac changes
Assesses potassium-related
cardiac changes
Do not wait for every lab to return before starting treatment when clinical suspicion is high.
Complications — and Why Speed Matters
Both conditions can cause severe complications. The mnemonic SHOCKED helps recall them:
Seizures, Hypovolemia, Organ failure, Cerebral edema, Kidney injury, Electrolyte imbalance,
Death.
Specific points worth emphasising:
Cerebral edema — more common in children with DKA; potentially fatal
Seizures — especially in HHS
Cardiac arrhythmias — from electrolyte imbalance, particularly potassium
Thrombosis — HHS increases blood viscosity and clot risk
Shock and acute kidney injury — from severe dehydration
Coma and death — mortality is higher in HHS overall
Delayed treatment increases mortality. With early recognition and aggressive management,
most patients recover successfully.
Management: Fluids First, Then Insulin
Both DKA and HHS are medical emergencies. Treatment goals include fluid replacement, insulin
therapy, electrolyte correction, and treating the underlying cause.
- Fluid resuscitation — the first and most important step. Intravenous fluids restore circulation
and hydration. - Insulin therapy — regular insulin reduces blood glucose and ketone production. Insulin is
essential in DKA; do not withhold it waiting for potassium results without a clear plan for
monitoring. - Potassium replacement — although serum potassium may initially appear high, total body
potassium is usually depleted. Careful monitoring is critical. - Correction of acidosis — usually improves with fluids and insulin; do not chase acidosis in
isolation. - Treat the underlying cause — antibiotics for infection, management of myocardial infarction,
adjustment of precipitating medications. - Monitoring — blood glucose, electrolytes, vital signs, and urine output require frequent
reassessment. Severe cases may need ICU admission.
A note for practice in Ghana
At district hospitals and polyclinics, you may stabilise and refer while treatment is underway. Do
not delay IV fluids and insulin while arranging transfer to a centre with intensive monitoring —
particularly for young DKA patients at risk of cerebral edema. Document glucose, ketones where
available, blood pressure, mental status, and urine output during transfer.
Prevention: Where the Real Battle Is Won
Education is extremely important — and in resource-limited settings, it is often the intervention we can actually deliver consistently.
Medication adherence — patients should never stop insulin abruptly
Sick day rules — continue insulin during illness and monitor glucose frequently; illness increases insulin requirements, not decreases them
Adequate hydration — especially important in elderly patients at risk of HHS
Early infection treatment — prompt management prevents deterioration
Regular follow-up — routine diabetes care reduces complications Recurrent diabetic emergencies carry psychological and social weight: anxiety, depression, financial burden, and reduced quality of life. Support and education are not optional extras —
they are part of treatment.
Key Takeaways
DKA and HHS are both medical emergencies arising from inadequate insulin activity and severe hyperglycemia
DKA features ketosis and metabolic acidosis; it commonly affects younger patients with type 1 diabetes
HHS features profound dehydration and hyperosmolarity with minimal ketosis; it typically affects older adults with type 2 diabetes
Infection and missed insulin are the most common triggers — ask about both immediately
Fluids first, then insulin, with careful potassium monitoring
Cerebral edema in paediatric DKA and severe neurological impairment in HHS demand urgent action
Prevention through sick-day education and adherence support saves lives
The teenager with fruity breath and Kussmaul respirations is not being dramatic. His body is compensating for acidosis while his cells starve for glucose. Recognise the pattern, start fluids, give insulin, find the trigger — and teach the family before discharge so the next crisis never happens.
For emergency diabetes care in Ghana, proceed to the nearest hospital with IV fluid and monitoring capacity. Type 1 diabetes patients and their families should receive sick-day education at every clinic visit. Health workers can contact teaching hospital endocrine and paediatric services for referral guidance when managing severe DKA or HHS.
Disclaimer
The information contained in this post is for general information purposes only. The information is provided by The Hidden Truth Behind DKA And HHS and while we endeavour to keep the information up to date and correct, we make no representations or warranties of any kind, express or implied, about the completeness, accuracy, reliability, suitability or availability with respect to the website or the information, products, services, or related graphics contained on the post for any purpose.