Medical disclaimer: This article is for general health education only. It does not replace
examination, diagnosis, or treatment by a qualified doctor. If you have chronic cough, worsening
breathlessness, chest tightness, or confusion with breathing difficulty, please seek care at your
nearest health facility.

The breath gets shorter. The cough stays. The damage, once done, does not fully undo itself.. In a village outside Sunyani, a woman in her late fifties cooks twice daily over a charcoal stove in a kitchen with one small window. She has never smoked a cigarette. For ten years she has coughed most mornings, bringing up white mucus. She thought it was “kitchen heat.” Now she
cannot walk to the market without stopping. At the health centre, the nurse hears prolonged expiration and reduced breath sounds. Spirometry — available that day through outreach — shows airflow obstruction that does not fully reverse after salbutamol.
This is chronic obstructive pulmonary disease: common, progressive, and in Ghana often tied as much to biomass smoke as to cigarettes.
COPD is a long-term respiratory disease characterised by persistent airflow limitation that gradually worsens over time. It is among the leading causes of illness and death worldwide and significantly affects quality of life. Although it cannot usually be completely cured, early diagnosis and proper management can slow progression, reduce symptoms, and improve daily
living.
What COPD Actually Is
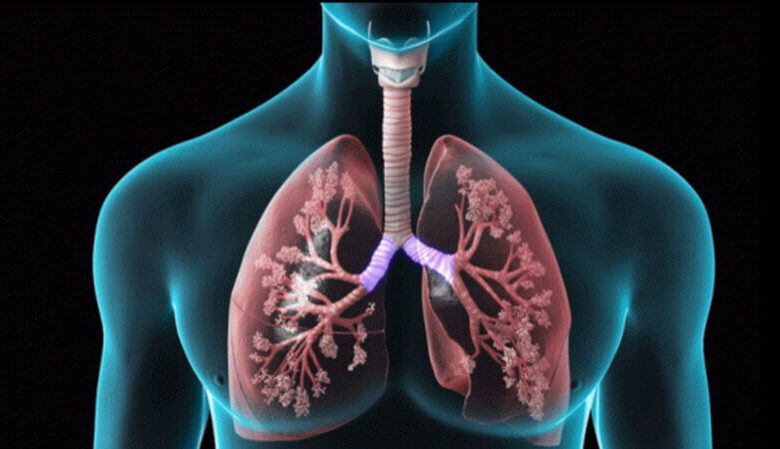
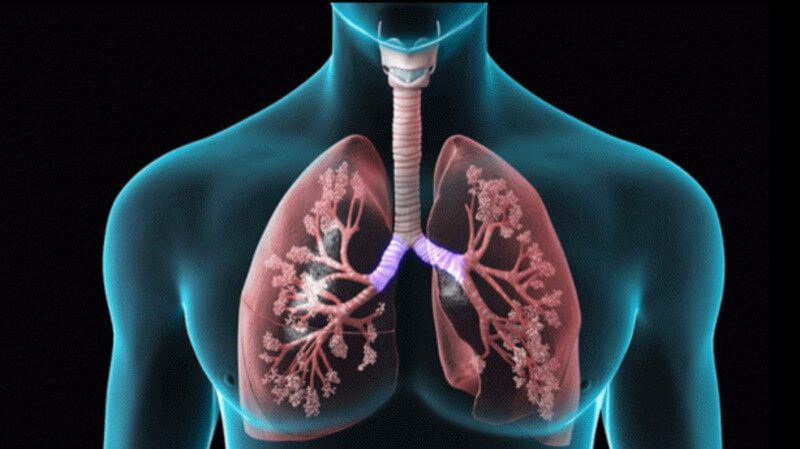
Chronic obstructive pulmonary disease is a chronic inflammatory lung disease with persistent airflow obstruction that is not fully reversible. It mainly comprises two overlapping conditions Chronic bronchitis — clinically defined as a productive cough lasting at least three months in each of two consecutive years, with excess mucus, chronic cough, and inflamed airways. Emphysema — destruction of alveoli leading to loss of lung elasticity, air trapping, and reduced gas exchange.
Many patients have features of both simultaneously. The disease develops slowly over years and is strongly associated with cigarette smoking, environmental pollution, occupational exposure to dust and fumes, and — critically in developing countries — indoor biomass fuel smoke. It mainly affects adults above 40 years; risk increases with age and cumulative exposure to
harmful particles and gases.
Causes And Risk Factors
COPD develops after long-term exposure to irritants that damage airways and alveoli.
Cigarette smoking remains the leading cause worldwide.
Active and passive smoking damage airways, alveoli, and lung defence mechanisms. Duration and intensity matter.
Biomass fuel exposure is common in developing countries.
Indoor cooking smoke from wood, charcoal, and animal dung in poorly ventilated homes damages lungs over decades.
In Ghana, this exposure deserves the same clinical weight as pack-years of cigarettes when taking history.
Occupational exposure to dust, chemicals, fumes, and industrial smoke increases risk — relevant for miners, factory workers, and agricultural labour without protection.
Air pollution, alpha-1 antitrypsin deficiency (a rare genetic cause of early emphysema), and recurrent childhood respiratory infections that impair lung development also contribute.
Long-standing poorly controlled asthma may overlap with or progress toward COPD.
Risk factors cluster usefully under SMOKED: Smoking, Mining/occupational exposure, Older age, Kitchen smoke, Environmental pollution, Deficiency of alpha-1 antitrypsin.
Poor socioeconomic conditions — malnutrition, pollution exposure, limited healthcare access —compound vulnerability. Ask not only “Do you smoke?” but “What do you cook with, and where?”
How Lung Damage Progresses
COPD Pathophysiology Is a Slow Cascade:
- Exposure to harmful irritants
- Chronic inflammation with inflammatory cells in airways
- Mucus hypersecretion
- Airway narrowing from inflammation and fibrosis
- Alveolar destruction in emphysema — walls break down, elastic recoil is lost
- Air trapping during exhalation
- Impaired gas exchange — falling oxygen, rising carbon dioxide
- Pulmonary hypertension from chronic hypoxia
- Right heart strain — cor pulmonale
Clinicians sometimes recall BLOCK AIR: Bronchial inflammation, Loss of alveoli, Obstructed
airflow, Chronic mucus production, Knocked-out gas exchange, Air trapping, Inflammation,
Respiratory failure.
Understanding the cascade explains why late presentation is costly: by the time breathlessness
is constant, much structural damage is already fixed.
Signs, Symptoms, and Exacerbations
Symptoms develop gradually over years.
Chronic cough — often earliest; usually productive
Sputum — white, yellow, or thick
Shortness of breath — initially on exertion, later at rest
Wheezing and chest tightness, especially during exacerbations
Fatigue from reduced oxygen delivery
Frequent respiratory infections
Weight loss in advanced disease
Cyanosis and swollen ankles suggesting right heart failure
On clinical Examinations
Examination may reveal barrel-shaped chest, use of accessory muscles, prolonged expiration,and reduced breath sounds.
Older textbooks describe pink puffers (emphysema-dominant: thin, breathless, minimal cyanosis) and blue bloaters (chronic bronchitis-dominant: cyanosis, oedema, productive cough).
These are educational stereotypes, not diagnoses — but they remind us that COPD phenotypes differ.
A symptom mnemonic: COUGH — Chronic cough, Obstructed breathing, Unable to exercise well, Gasping for air, Heavy sputum production.
Exacerbations
An exacerbation is sudden worsening — often triggered by infection, pollution, or continued
smoking. Symptoms escalate rapidly. Severe exacerbation warning signs include severe
breathlessness, confusion, cyanosis, drowsiness, and respiratory distress. These are
emergencies.
Diagnosis: History Plus Spirometry
Diagnosis combines history, examination, and investigations.
History should document smoking, occupational exposure, biomass smoke, and chronic respiratory symptoms.
Examination looks for wheeze, hyperinflation, and cyanosis.
Spirometry is the most important diagnostic test, measuring airflow obstruction.
COPD is diagnosed when airflow limitation persists after bronchodilator use and is not fully reversible — distinguishing it from asthma alone.
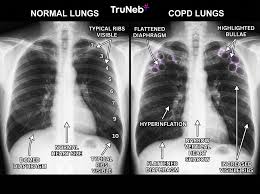
Chest X-ray may show hyperinflated lungs and flattened diaphragm. CT evaluates emphysema in more detail. Arterial blood gas and pulse oximetry assess oxygenation and carbon dioxide retention.
Sputum analysis helps during infections. ECG and echocardiography evaluate cardiac complications.
Severity is often described as mild (symptoms mainly on exertion), moderate (worsening breathlessness), severe (frequent exacerbations, limited activity), and very severe (respiratory failure risk).
Spirometry and symptom burden together guide management — not either alone.
Complications Across The Body
COPD is a lung disease that becomes a whole-body disease.
Respiratory failure.
Recurrent pneumonia.
Pulmonary hypertension.
Cor pulmonale.
Pneumothorax from rupture of damaged alveoli. Weight loss and muscle wasting.
Depression and anxiety. Osteoporosis from inactivity and steroid exposure.
Sleep disturbance from hypoxia.
Increased mortality in severe disease.
BREATHLESS captures much of this: Bronchial infections, Respiratory failure, Edema/cor pulmonale, Anxiety, Tension pneumothorax, Hypoxia, Loss of weight, Exercise intolerance, Sleep disturbance, Secondary osteoporosis. Breathlessness shrinks social life. Patients stop attending gatherings. Isolation deepens depression. Treat the mind alongside the lungs.
Management: What Actually Changes Outcomes
COPD management aims to relieve symptoms, improve quality of life, reduce exacerbations, and slow progression.
Smoking cessation is the most important intervention — including reducing exposure to passive smoke and, where possible, changing cooking practices to cleaner fuels and better ventilation.
Stopping smoking slows lung damage even after COPD is established.
Pharmacological treatment includes:
Bronchodilators — salbutamol, tiotropium — relax airway smooth muscle
Inhaled corticosteroids — budesonide and others reduce inflammation
Combination inhalers pairing bronchodilators and steroids
Antibiotics during bacterial exacerbations
Long-term oxygen for chronic severe hypoxemia
Vaccination against influenza and pneumococcus
Pulmonary rehabilitation — exercise training, education, nutritional counselling — improves exercise tolerance and quality of life even when spirometry numbers barely move.
Nutritional support with adequate protein matters in wasting. Breathing techniques such as pursed-lip and diaphragmatic breathing help some patients day to day.
Surgical options for selected severe cases include lung volume reduction surgery, bullectomy, and lung transplantation.
Acute exacerbation management may require oxygen, bronchodilators, steroids, antibiotics, and non-invasive ventilation in severe respiratory distress.
A management mnemonic: BREATHE — Bronchodilators, Rehabilitation, Exercise, Avoid smoking, Treat infections, Home oxygen, Education.
In Ghanaian practice, the practical barriers are familiar: inhaler cost, spacer availability, distance to rehabilitation, and patients who were never told biomass exposure counts. Address exposure in the consultation with the same seriousness as cigarettes.
Prevention and Prognosis
Prevention priorities: avoid smoking, reduce occupational exposure with protective equipment, improve indoor ventilation to reduce kitchen smoke, vaccinate, and treat respiratory illness early to preserve lung function.
COPD is progressive, but outcomes vary with smoking cessation, severity, exacerbation frequency, and oxygen levels.
Early diagnosis improves long-term trajectory even when lung function cannot be restored to normal.
Public awareness matters — not to frighten, but to move people from “normal cough of age” to
spirometry before disability settles.
What Patients, Families, and Clinicians Should Know
If you cook with charcoal or wood in a closed kitchen and cough year after year, that history belongs in a medical record. If you are breathless walking distances you once managed easily, ask for spirometry. If you use an inhaler, learn technique — poor inhaler use is wasted medicine.
If you are a health worker: take a fuel and occupation history alongside smoking pack-years.
Refer exacerbations with altered consciousness or severe distress urgently. Vaccinate eligible patients when vaccines are available. Celebrate smoking cessation and cleaner cooking — both are clinical interventions.
COPD is irreversible airflow limitation. That truth is sobering. It is not the whole story. Many
patients with proper treatment breathe easier, stay out of hospital longer, and live fuller lives
than they imagined at diagnosis.
Key Takeaways
COPD is persistent, not fully reversible airflow obstruction — chronic bronchitis and
emphysema often coexist
Cigarette smoking is the leading cause globally; biomass kitchen smoke is a major
contributor in Ghana
Chronic cough, sputum, exertional breathlessness, and recurrent infections are core
symptoms
Spirometry after bronchodilator is essential for diagnosis
Smoking cessation and reduced smoke exposure slow progression; rehabilitation and
inhalers reduce symptoms
Exacerbations with confusion, cyanosis, or severe distress need urgent care
Partial success is the realistic goal: one fewer exacerbation this year, a patient who switches to a
better-ventilated cook space, oxygen saturation stable enough to sleep lying flat. Those wins are
worth pursuing from the first honest history about the kitchen.
For chronic cough and breathlessness, seek assessment at your nearest health facility. Ask about spirometry and inhaler technique. If you use biomass fuels for cooking, improve ventilation where possible and discuss cleaner alternatives with your local health education team.
Disclaimer
The information contained in this post is for general information purposes only. The information is provided by COPD Is Not Only An Irreversible Smoker's Disease and while we endeavour to keep the information up to date and correct, we make no representations or warranties of any kind, express or implied, about the completeness, accuracy, reliability, suitability or availability with respect to the website or the information, products, services, or related graphics contained on the post for any purpose.



