Introduction
Non-Hodgkin’s lymphoma (NHL) is a broad group of cancers that comes from the lymphatic system, specifically from lymphocytes, which are a type of white blood cell that is responsible for the human immune defense system. It is one of the most common hematological malignancies worldwide and affects both adults and children, although it is more frequent in older adults. Unlike Hodgkin’s lymphoma, Non-Hodgkin’s lymphoma includes many subtypes that vary in behavior, treatment response, and prognosis. so what are the differences between these two conditions.
Difference Between Hodgkin’s Lymphoma and Non-Hodgkin’s Lymphoma
Lymphoma is a cancer of the lymphatic system. It is broadly divided into Hodgkin’s lymphoma (HL) and Non-Hodgkin’s lymphoma (NHL). Although both arise from lymphocytes, they differ in pathology, spread, symptoms, treatment response, and prognosis.
Quick Comparison Table
| Feature | Hodgkin’s Lymphoma | Non-Hodgkin’s Lymphoma |
|---|---|---|
| Definition | Malignant lymphoma characterized by presence of Reed-Sternberg cells | Group of lymphoid cancers without Reed-Sternberg cells |
| Cell of Origin | Usually B lymphocytes | B cells, T cells, or NK cells |
| Characteristic Cell | Reed-Sternberg giant cells present | Reed-Sternberg cells absent |
| Age Group | Common in young adults and older adults (bimodal peak) | More common in older adults, but can occur at any age |
| Pattern of Spread | Spreads in an orderly, contiguous manner from one lymph node group to another | Often spreads unpredictably and non-contiguously |
| Lymph Node Involvement | Usually starts in cervical or mediastinal nodes | Can start in many lymph node groups |
| Extranodal Disease | Less common | More common (GIT, skin, brain, bone marrow, etc.) |
| Number of Types | Fewer subtypes | Many subtypes |
| Common Symptoms | Painless lymphadenopathy, fever, night sweats, weight loss | Same symptoms plus more extranodal symptoms |
| Prognosis | Generally very good, high cure rate | Depends on subtype; some curable, some chronic |
| Treatment | Chemotherapy ± radiotherapy | Chemotherapy, immunotherapy, targeted therapy, radiotherapy |
| Examples | Nodular sclerosis HL, Mixed cellularity HL | Diffuse large B-cell lymphoma, Follicular lymphoma, Burkitt lymphoma |
Detailed Difference
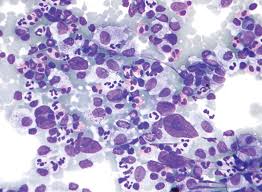
1. Presence of Reed-Sternberg Cells
This is the most important distinction.
- Hodgkin’s lymphoma: Contains large abnormal Reed-Sternberg cells seen on biopsy.
- Non-Hodgkin’s lymphoma: Does not contain Reed-Sternberg cells.
2. Pattern of Spread
- Hodgkin’s lymphoma: Usually spreads from one lymph node region to the next nearby region.
- Non-Hodgkin’s lymphoma: May skip areas and spread widely early.
3. Extranodal Involvement
- Hodgkin’s lymphoma: Mainly remains in lymph nodes.
- Non-Hodgkin’s lymphoma: Frequently affects organs outside lymph nodes such as stomach, intestines, skin, CNS, or marrow.
4. Types of Cells Involved
- Hodgkin’s lymphoma: Mostly B-cell origin.
- Non-Hodgkin’s lymphoma: Can arise from B-cells, T-cells, or NK cells.
5. Prognosis
- Hodgkin’s lymphoma: One of the most curable cancers, especially early stages.
- Non-Hodgkin’s lymphoma: Outcome varies widely depending on subtype and stage.
6. Common Sites
- Hodgkin’s lymphoma: Neck nodes, mediastinum.
- Non-Hodgkin’s lymphoma: Any lymph node group or extranodal tissue.

Memory Trick
Hodgkin’s = Has Reed-Sternberg cells
Non-Hodgkin’s = No Reed-Sternberg cells
Definition
Non-Hodgkin’s lymphoma is a malignant disorder characterized by uncontrolled proliferation of lymphoid cells, mainly B lymphocytes, T lymphocytes, or natural killer (NK) cells, occurring in lymph nodes or extranodal lymphoid tissues. It represents all lymphomas that do not show the classical Reed-Sternberg cells seen in Hodgkin’s lymphoma.
NHL is not a single disease but a collection of many distinct lymphoid malignancies, classified according to the type of cell involved, genetic features, and growth pattern.
Examples include:
- Diffuse large B-cell lymphoma (DLBCL)
- Follicular lymphoma
- Burkitt lymphoma
- Mantle cell lymphoma
- Marginal zone lymphoma
- Peripheral T-cell lymphoma
- Cutaneous T-cell lymphoma
Aetiology (Causes and Risk Factors)
The exact cause of Non-Hodgkin’s lymphoma is not fully understood, but several factors are known to increase the risk.
1. Genetic Mutations
Changes in DNA within lymphocytes can cause abnormal growth and resistance to cell death. These mutations may occur spontaneously or due to environmental exposure.
Examples include:
- t(14;18) translocation in follicular lymphoma
- c-MYC translocation in Burkitt lymphoma
- BCL6 abnormalities in diffuse large B-cell lymphoma
2. Immunodeficiency States
People with weakened immune systems are at higher risk.
Examples:
- HIV/AIDS
- Congenital immunodeficiency disorders
- Post-organ transplant immunosuppression
- Long-term use of immunosuppressive drugs
3. Autoimmune Diseases
Chronic immune stimulation may predispose to lymphoma.
Examples:
- Rheumatoid arthritis
- Sjögren syndrome
- Systemic lupus erythematosus
- Hashimoto thyroiditis
4. Infections
Certain infections are associated with specific lymphoma subtypes.
- Epstein-Barr virus (EBV): Burkitt lymphoma, some aggressive lymphomas
- Helicobacter pylori: Gastric MALT lymphoma
- Hepatitis C virus: Marginal zone lymphoma
- Human T-cell leukemia virus type 1 (HTLV-1): Adult T-cell lymphoma
- Human herpesvirus 8 (HHV-8): Primary effusion lymphoma
5. Environmental and Occupational Exposure
- Pesticides
- Herbicides
- Benzene
- Radiation exposure
- Certain industrial chemicals
6. Age and Gender
- Incidence increases with age
- Slight male predominance in many subtypes
7. Family History
Having a close relative with lymphoma or hematological cancer may slightly increase risk.
Pathophysiolog
Non-Hodgkin’s lymphoma develops when lymphocytes undergo malignant transformation. Normally, lymphocytes grow, mature, perform immune functions, and die in an organized manner. In NHL, mutations disrupt this balance.
Stepwise Mechanism
1. Genetic Damage
DNA mutations or chromosomal translocations occur in B-cells, T-cells, or NK cells.
2. Loss of Growth Control
Mutated cells begin to multiply uncontrollably and evade apoptosis (programmed cell death).
3. Clonal Expansion
The abnormal cell reproduces identical malignant cells, forming a clone.
4. Tissue Infiltration
Cancer cells accumulate in:
- Lymph nodes
- Bone marrow
- Spleen
- Liver
- Gastrointestinal tract
- Skin
- Central nervous system
5. Immune Dysfunction
Normal lymphocyte production is impaired, leading to recurrent infections and reduced immunity.
6. Organ Damage
Large tumor masses or diffuse infiltration interfere with organ function.
Classification
NHL can be broadly divided into:
A. Indolent (Slow Growing)
- Follicular lymphoma
- Small lymphocytic lymphoma
- Marginal zone lymphoma
These may remain stable for years but can relapse repeatedly.
B. Aggressive (Fast Growing)
- Diffuse large B-cell lymphoma
- Mantle cell lymphoma
- Peripheral T-cell lymphoma
Require urgent treatment.
C. Highly Aggressive
- Burkitt lymphoma
- Lymphoblastic lymphoma
Rapid progression but often responsive to intensive therapy.
Signs and Symptoms
Clinical presentation depends on subtype, site, and stage.
1. Lymphadenopathy
Most common feature.
- Enlarged lymph nodes
- Usually painless
- Common in neck, axilla, groin
Nodes may be firm, rubbery, and persistent.
2. Constitutional (B) Symptoms
These suggest systemic disease:
- Unexplained fever
- Drenching night sweats
- Weight loss (>10% body weight in 6 months)
3. Fatigue and Weakness
Due to anemia, cytokine release, or chronic disease.
4. Recurrent Infections
From impaired immune function.
5. Extranodal Symptoms
Gastrointestinal Involvement
- Abdominal pain
- Nausea
- Vomiting
- Bowel obstruction
- GI bleeding
CNS Involvement
- Headache
- Seizures
- Weakness
- Personality changes
Skin Involvement
- Nodules
- Plaques
- Itching
Bone Marrow Involvement
- Pallor
- Easy bruising
- Bleeding
- Infections
6. Hepatosplenomegaly
Enlarged liver or spleen may cause abdominal fullness.
7. Mediastinal Mass
May cause:
- Cough
- Chest pain
- Dyspnea
- Superior vena cava obstruction
Investigations to Do as a Doctor
Proper diagnosis requires a systematic approach.
1. Full Clinical Assessment
- History of symptoms duration
- Weight loss, fever, sweats
- Exposure history
- HIV risk factors
- Autoimmune disease history
- Drug history
2. Physical Examination
- Lymph node regions
- Liver and spleen size
- Skin lesions
- Signs of anemia
- Neurological assessment
Laboratory Investigations
3. Complete Blood Count (CBC)
May reveal:
- Anemia
- Leukopenia
- Leukocytosis
- Thrombocytopenia
4. Peripheral Blood Film
May show abnormal lymphoid cells.
5. ESR / CRP
Markers of inflammation.
6. LDH (Lactate Dehydrogenase)
Often elevated in aggressive disease and high tumor burden.
7. Uric Acid
May be elevated due to rapid cell turnover.
8. Liver Function Tests
Assess liver involvement and chemotherapy readiness.
9. Renal Function Tests
Important before treatment.
10. Viral Screening
- HIV
- Hepatitis B
- Hepatitis C
Tissue Diagnosis
11. Excisional Lymph Node Biopsy
Gold standard investigation.
A whole node is removed for:
- Histology
- Immunohistochemistry
- Flow cytometry
- Cytogenetics
Fine needle aspiration alone is usually insufficient.
12. Bone Marrow Aspiration and Trephine Biopsy
Used for staging and marrow involvement.
Imaging Studies
13. Chest X-ray
Detect mediastinal mass.
14. CT Scan
Neck, chest, abdomen, pelvis for staging.
15. PET-CT Scan
Useful for:
- Disease extent
- Response assessment
- Detecting residual active disease
16. MRI
Used for CNS, spine, or soft tissue involvement.
Special Tests
17. Lumbar Puncture
If CNS involvement suspected.
18. Molecular Studies
Detect genetic abnormalities and guide prognosis.
Staging
Ann Arbor staging system is commonly used:
- Stage I: Single lymph node region or single extranodal site
- Stage II: Two or more lymph node regions on same side of diaphragm
- Stage III: Both sides of diaphragm involved
- Stage IV: Disseminated extranodal disease (bone marrow, liver, CNS)
Suffixes:
- A = no B symptoms
- B = fever, sweats, weight loss
Complications
Non-Hodgkin’s lymphoma can produce many complications.
Disease-Related Complications
1. Bone Marrow Failure
Causing:
- Severe anemia
- Infection
- Bleeding
2. Organ Compression
Tumor masses may compress:
- Airways
- Ureters
- Blood vessels
- Spinal cord
3. CNS Spread
Neurological deficits and seizures.
4. Intestinal Obstruction or Perforation
Especially with abdominal lymphoma.
5. Hypercalcemia
Occasionally seen in some subtypes.
6. Tumor Lysis Syndrome
Rapid destruction of cancer cells causing:
- Hyperuricemia
- Hyperkalemia
- Hyperphosphatemia
- Renal failure
Treatment-Related Complications
7. Neutropenic Sepsis
Medical emergency after chemotherapy.
8. Cardiotoxicity
Some drugs (e.g., doxorubicin) can damage heart.
9. Infertility
Following chemotherapy/radiotherapy.
10. Secondary Malignancies
Long-term risk after treatment.
Management
Treatment depends on:
- Histological subtype
- Stage
- Age
- Performance status
- Organ function
- Presence of symptoms
Management is best coordinated by a hematologist/oncologist.
1. Supportive Care
Essential in all patients.
- Adequate nutrition
- Pain control
- Hydration
- Infection prevention
- Psychological support
- Blood transfusion if needed
2. Watchful Waiting
Used in selected indolent lymphomas without symptoms.
Patients are monitored regularly until treatment becomes necessary.
3. Chemotherapy
Mainstay for many forms of NHL.
Common Regimen: R-CHOP
Used for diffuse large B-cell lymphoma.
Includes:
- Rituximab
- Cyclophosphamide
- Doxorubicin
- Vincristine
- Prednisolone
Other regimens depend on subtype.
4. Immunotherapy
Rituximab
Monoclonal antibody against CD20 on B-cells.
Often combined with chemotherapy.
Other newer antibodies are also available.
5. Targeted Therapy
Used in relapsed or specific subtypes.
Examples:
- Ibrutinib
- Acalabrutinib
- Venetoclax
- Lenalidomide
6. Radiotherapy
Useful for:
- Localized early-stage disease
- Bulky masses
- Palliation of pain or compression
7. Stem Cell Transplant
For relapsed or high-risk disease.
Autologous transplant
Uses patient’s own stem cells.
Allogeneic transplant
Uses donor stem cells.
8. CAR T-Cell Therapy
Advanced treatment for some refractory B-cell lymphomas.
Patient’s T-cells are modified to attack lymphoma cells.
9. Management of Complication
Tumor Lysis Syndrome
- IV fluids
- Allopurinol
- Rasburicase
- Electrolyte correction
Febrile Neutropenia
- Immediate IV antibiotics
- Cultures
- Supportive care
Spinal Cord Compression
- Emergency steroids
- MRI
- Radiotherapy or surgery
Prognosis
Outcome depends on subtype and stage.
Indolent lymphomas may be chronic but manageable for years.
Aggressive lymphomas can often be cured if treated early.
Poor prognostic factors include:
- Advanced age
- High LDH
- Poor performance status
- Advanced stage
- Multiple extranodal sites
The International Prognostic Index (IPI) helps risk stratification.
Prevention
There is no guaranteed prevention, but risk may be reduced by:
- HIV prevention and treatment
- Avoiding unnecessary chemical exposure
- Managing autoimmune diseases
- Treating chronic infections such as H. pylori
- Regular medical review of persistent lymph node swelling
When to Suspect NHL as a Doctor
A doctor should consider Non-Hodgkin’s lymphoma when a patient presents with:
- Persistent painless lymph node enlargement
- Unexplained weight loss
- Night sweats
- Fever of unknown origin
- Hepatosplenomegaly
- Recurrent infections
- Unexplained cytopenias
- Mass lesions in extranodal sites
Prompt biopsy is essential.
Conclusion
Non-Hodgkin’s lymphoma is a diverse group of malignant diseases of the lymphoid system ranging from slow-growing conditions to rapidly fatal cancers if untreated. Because it can mimic infections or benign lymph node enlargement, a high index of suspicion is required in clinical practice. Early diagnosis through biopsy, laboratory tests, and imaging allows timely treatment and significantly improves survival.
Modern therapy now combines chemotherapy, immunotherapy, radiotherapy, targeted drugs, and cellular therapies, making many forms of Non-Hodgkin’s lymphoma highly treatable and in some cases curable. For healthcare professionals, careful assessment, accurate staging, and individualized treatment planning remain the key pillars of management.
Disclaimer
The information contained in this post is for general information purposes only. The information is provided by Non-Hodgkin’s Lymphoma: A Comprehensive Educational Review and while we endeavour to keep the information up to date and correct, we make no representations or warranties of any kind, express or implied, about the completeness, accuracy, reliability, suitability or availability with respect to the website or the information, products, services, or related graphics contained on the post for any purpose.