Medical disclaimer: This article is for general health education only. It does not replace examination, diagnosis, or treatment by a qualified doctor. If you have persistent cough, breathlessness, coughing up blood, or worsening chest symptoms, please seek care at your nearest health facility.
When the Cough Never Really Leaves —Bronchiectasis and Atelectasis, One is a damaged airway that cannot clear itself. The other is a lung that has simply stopped opening.
A man in his fifties sits in the outpatient department at a district hospital in Tamale, holding a plastic bag of his morning sputum. He has had a productive cough for years — thick, yellow- green, sometimes foul-smelling. He was treated for tuberculosis as a young man and assumed the lungs had healed. They did heal, in a sense. But the airways did not return to normal. Across the ward, a woman who had abdominal surgery three days ago is breathing shallowly, wincing when the nurse asks her to take a deep breath. Her oxygen saturation is drifting down.
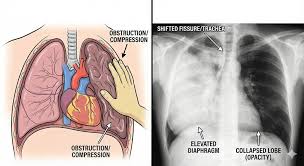
The chest X-ray shows a patch of collapsed lung at the base — not infection, not pneumonia at first glance, but atelectasis. These two presentations look alike from the waiting room: cough, chest discomfort, breathlessness. Clinically, they are different problems requiring different thinking. Confusing them wastes time. Recognising each early protects lung function.
Bronchiectasis: Airways That Stay Damaged
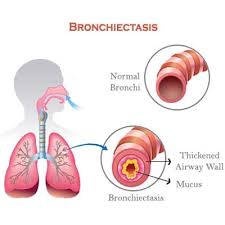
Bronchiectasis is a chronic lung disease defined by permanent abnormal dilation and destruction of the bronchi, caused by repeated inflammation and infection. The damaged airways widen, lose their normal architecture, and fail to clear mucus effectively.Once mucus stagnates, bacteria grow easily. Recurrent infections follow. Each episode inflames and injures the bronchial walls further. The cycle becomes self-perpetuating.
In Ghana, tuberculosis history matters enormously. TB is among the most important causes of bronchiectasis worldwide — alongside severe pneumonia, severe childhood respiratory infections, cystic fibrosis (more prominent in developed countries), COPD, immune deficiency, repeated aspiration, airway obstruction from tumours or foreign bodies, autoimmune disease such as rheumatoid arthritis or lupus, and allergic bronchopulmonary aspergillosis.
The condition can occur at any age but is more common in older adults, patients with chronic lung disease, and those with recurrent infections. Improved imaging has increased recognition globally — which means more patients who were once labelled as “chronic bronchitis” or “post- TB lung” may finally receive a precise diagnosis. How bronchiectasis develops Think of the pathophysiology as a staircase:
- Airway injury — infection, obstruction, or inflammation damages bronchi
- Impaired mucus clearance — damaged cilia cannot sweep secretions upward
- Mucus accumulation — secretions pool in widened airways
- Bacterial growth — stagnant mucus becomes a culture medium
- Chronic inflammation — persistent inflammation destroys bronchial walls
- Permanent airway dilation — bronchi become widened, distorted, and scarred
Clinicians sometimes remember this cycle with MUCUS: Mucus retention, Uncontrolled infection, Chronic inflammation, Unhealthy bronchi, Structural airway damage. What patients report.
The hallmark is chronic productive cough — often the most common and most overlooked symptom. Patients may bring impressive volumes of sputum: thick, yellow, green, foul-smelling. Other features include recurrent chest infections requiring frequent antibiotics, gradually worsening shortness of breath, wheezing, hemoptysis, fatigue, chest pain during infections, and
finger clubbing from chronic hypoxia.
A useful symptom mnemonic is COUGH: Chronic cough,
Ongoing infections,
Unpleasant sputum,
Gasping for air,
Hemoptysis.
Listen for the pattern: years of symptoms, seasons of worsening, a history of severe lung infection in youth or adulthood. In a patient who completed TB treatment decades ago but never stopped coughing, bronchiectasis should be on your differential.
Diagnosis and complications. History should explore chronic cough, recurrent infections, and sputum character. Examination
may reveal crackles, wheezing, and clubbing. Chest X-ray may suggest airway abnormalities, but high-resolution CT is the best diagnostic test — it shows dilated bronchi clearly. Sputum culture identifies infecting organisms. Spirometry evaluates lung function. Blood tests may assess immune status and inflammation. Untreated bronchiectasis can lead to recurrent pneumonia, massive hemoptysis, respiratory failure, pulmonary hypertension, cor pulmonale, and lung abscess.
Management and prevention
Treatment aims to control infection, improve mucus clearance, and preserve lung function.
Antibiotics during exacerbations, guided by sputum culture where possible
Airway clearance techniques — chest physiotherapy is central
Bronchodilators such as salbutamol when airflow limitation is present
Mucolytics to thin secretions
Vaccination against influenza and pneumococcus
Oxygen therapy in severe hypoxia
Surgery for severe localised disease in selected cases
Prevention emphasises early treatment of infections, vaccination, smoking cessation, and proper asthma management. For Ghanaian practice, completing TB treatment is essential — but follow-up matters too. Ask whether cough persisted after cure. Document post-TB lung disease.
Refer for CT when chronic productive cough continues after adequate TB therapy.

Atelectasis: When Lung Tissue Collapses
Atelectasis is partial or complete collapse of lung tissue, with reduced or absent air in the alveoli. Gas exchange falls. Oxygenation suffers. Unlike bronchiectasis, atelectasis is not primarily a disease of permanently widened airways. It is a problem of ventilation — air failing to reach alveoli, or external forces compressing lung tissue shut.
Types and causes
Obstructive atelectasis follows airway blockage — mucus plugs, tumours, foreign bodies.
Compression atelectasis results from external pressure, such as pleural effusion.
Adhesive atelectasis occurs with surfactant deficiency, common in premature infants.
Postoperative atelectasis is familiar on surgical wards: pain leads to shallow breathing, alveoli collapse quietly at the bases.
Other causes include chest or abdominal surgery, pneumothorax, prolonged bed rest, sedation or anaesthesia, and neurological disease weakening respiratory muscles.
Risk factors include advanced age, smoking, recent surgery (especially thoracic or abdominal), chronic lung disease such as COPD or asthma, obesity, and neurological impairment.
Remember POST OP: Pain after surgery, Obesity, Smoking, Thoracic surgery, Obstruction, Prolonged bed
rest. Pathophysiology
The sequence is rapid compared with bronchiectasis:
- Reduced ventilation — air fails to reach alveoli
- Alveolar collapse
- Reduced gas exchange
- Hypoxemia
- Increased infection risk in collapsed segments
The mnemonic COLLAPSE captures this:
Collapse of alveoli,
Obstruction,
Low oxygen,
Loss of ventilation,
Air absorption,
Postoperative state,
Shallow breathing,
Effusion or external pressure.
Presentation and diagnosis
Small atelectasis may be asymptomatic. Larger collapse causes shortness of breath, rapid breathing, chest pain especially on deep inspiration, dry cough (often postoperative), low oxygen levels with possible cyanosis, fever if infection supervenes, and reduced breath sounds over the affected area.
Chest X-ray is the main diagnostic tool, showing collapse and possible shift of structures. CT provides detail. Pulse oximetry tracks oxygen saturation. Bronchoscopy is valuable when obstruction is suspected — it can remove mucus plugs or foreign bodies.
Complications include pneumonia in collapsed segments, respiratory failure, severe hypoxemia, sepsis from untreated infection, and permanent lung damage with fibrosis from chronic collapse.
Management and prevention
Treatment depends on cause:
Deep breathing exercises and incentive spirometry
Chest physiotherapy
Early mobilisation after surgery
Bronchoscopy for obstruction
Oxygen for hypoxemia
Treating underlying causes — draining effusions, managing tumours, treating infection
Prevention on surgical wards is not optional: deep breathing after surgery, adequate pain , control, early mobilisation, smoking cessation, and chest physiotherapy. In district hospitals where nurse-to-patient ratios are stretched, postoperative atelectasis is often preventable — and commonly missed until fever and tachypnea force attention.
How to Tell Them Apart
Both conditions may cause cough, breathlessness, chest discomfort, and recurrent respiratory problems. Both can progress to respiratory failure if ignored. But the clinical centre of gravity differs.
Feature Bronchiectasis Atelectasis
Main problem Airway dilation Lung collapse
Typical cause Chronic infection/inflammation
Obstruction, compression, shallow breathing , Sputum Large amounts, often purulent
Usually minimal
Course Chronic Acute or chronic
Best imaging HRCT showing dilated bronchi
Chest X-ray showing
collapsed segment
Defining symptom Chronic productive cough Breathlessness, especially postoperative Bronchiectasis asks: Why has this airway been injured repeatedly? Atelectasis asks: Why is this lung not expanding now?
Psychological and Social Impact
Chronic respiratory symptoms affect daily activities, sleep, employment, and emotional health.
Patients with years of productive cough may feel embarrassed, exhausted, or resigned.
Postoperative patients with hypoxia may panic, especially when breathlessness spikes at night.
Anxiety and depression are not secondary concerns — they influence adherence to physiotherapy, follow-up attendance, and smoking cessation. Acknowledge the burden directly.
What Patients and Clinicians Should Take Away
If you are a patient living with a cough that produces cupfuls of sputum, especially after TB or repeated pneumonias, you deserve imaging beyond a single chest X-ray when symptoms persist. Ask about HRCT referral. Ask about airway clearance techniques. Complete vaccinations. Do not accept “just live with it” if infections are recurrent.
If you are recovering from surgery and staff tell you to “take deep breaths,” that instruction is medicine — not politeness. Pain control matters because it enables expansion. Early walking matters. Incentive spirometry matters. If you are a clinician in Ghana — at a CHPS compound, polyclinic, district hospital, or teaching centre — keep both conditions in mind when lungs misbehave:
Chronic productive cough with infection history → think bronchiectasis; order CT when available
Recent surgery, shallow breathing, basal opacity → think atelectasis; mobilise and clear early
Chest physiotherapy helps both
Smoking worsens both
Key Takeaways
Bronchiectasis is permanent bronchial dilation from repeated infection and inflammation; TB history is a major cause in Ghana
Atelectasis is alveolar collapse from obstruction, compression, surfactant deficiency, or shallow postoperative breathing
HRCT is the best test for bronchiectasis; chest X-ray is the main tool for atelectasis
Chronic productive cough distinguishes bronchiectasis; postoperative hypoxia should trigger atelectasis thinking
Airway clearance, early mobilisation, infection control, and smoking cessation improve outcomes for both
Success is often partial but meaningful: fewer admissions, better oxygen saturation after surgery, a patient with post-TB bronchiectasis who finally understands why the cough never stopped. That clarity is worth the careful question and the correct scan.
For persistent respiratory symptoms or postoperative breathing difficulty, seek evaluation at your nearest health facility. If bronchiectasis is suspected after TB or recurrent pneumonia, ask your clinician about referral for high-resolution CT and physiotherapy-led airway clearance.
Disclaimer
The information contained in this post is for general information purposes only. The information is provided by Overview Of Bronchiectasis And Atelectasis and while we endeavour to keep the information up to date and correct, we make no representations or warranties of any kind, express or implied, about the completeness, accuracy, reliability, suitability or availability with respect to the website or the information, products, services, or related graphics contained on the post for any purpose.