Medical disclaimer: This article is for general health education only. It does not replace examination, diagnosis, or treatment by a qualified doctor. If you are on dialysis or have a fistula that feels different — no vibration, new swelling, pain, redness, or fever — seek care at your nearest health facility without delay.
At a renal unit in Accra, a nurse places two fingers over a patient’s inner forearm before the morning dialysis session. The skin is warm. A faint vibration travels through her fingertips — a thrill. She lifts her stethoscope and hears a continuous whoosh: the bruit. The vein along the wrist is visibly enlarged. These are not incidental findings. They mean the arteriovenous fistula is working. For patients with end-stage kidney disease, that surgically created connection between artery and vein is often the difference between reliable hemodialysis and repeated access emergencies.
In Ghana, where chronic kidney disease from diabetes and hypertension is increasingly seen at district hospitals and teaching centres alike, understanding fistulas matters for nurses, medical officers, surgeons, and the patients who live with one arm set aside for needles.
When the Kidneys Fail for Good
End-stage kidney disease — also called end-stage renal disease — is permanent, severe loss of kidney function. The kidneys can no longer maintain normal body functions. Waste products accumulate. Fluid balance breaks down. Electrolytes drift out of range.
At this stage, patients usually require renal replacement therapy: hemodialysis, peritoneal dialysis, or kidney transplantation. Hemodialysis removes waste and excess fluid by circulating blood through a machine. For that to work, large volumes of blood must move rapidly and reliably through vascular access. Among the three major access types — arteriovenous fistula, arteriovenous graft, and central venous catheter — the AV fistula is generally considered the best and safest option for many patients.
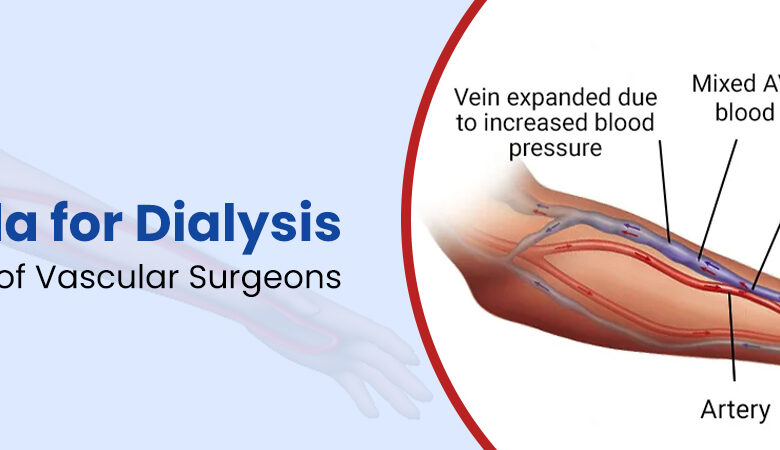
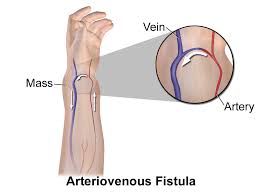
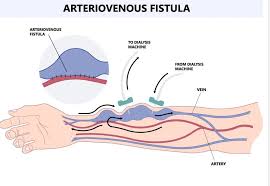
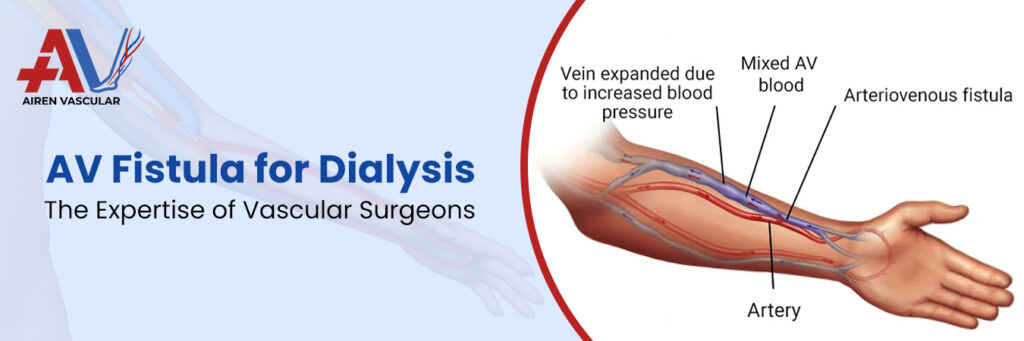
An arteriovenous fistula is a surgically created connection between an artery and a vein, usually in the arm, designed specifically for hemodialysis access. Blood flows directly from the high- pressure artery into the vein. Over weeks, the vein enlarges, thickens, and strengthens — a process called maturation — until it can tolerate repeated needle insertions and high blood flow rates during dialysis.
Why Fistulas Win Over Grafts and Catheters
The comparison is not abstract. AV fistulas use the patient’s own vessels, not synthetic material.
They carry lower infection risk, deliver better blood flow, last longer, clot less often, and allow
more efficient dialysis than grafts or catheters.
Feature AV Fistula AV Graft Central Venous
Catheter
Material Patient’s vessels Synthetic tube Tube in large vein
Infection risk Lower Higher Highest
Lifespan Longer Shorter Short-term use
Maturation 6–12 weeks Shorter Immediate but temporary
Blood flow Better Moderate Variable
For a patient travelling from a district hospital to a regional or teaching-centre dialysis unit under NHIS or out-of-pocket arrangements, a functioning fistula reduces the infections and access failures that already strain time, money, and referral pathways.
What Sends Patients Toward Dialysis — and Fistula Creation AV fistulas are created because severe kidney failure makes dialysis necessary. The underlying diseases are familiar in Ghanaian outpatient clinics. Diabetic nephropathy remains the leading cause worldwide. Long-standing hypertension damages kidney blood vessels. Chronic glomerulonephritis gradually destroys kidney filters. Polycystic kidney disease, lupus nephritis, obstructive uropathy, and recurrent kidney infections all appear on the list.
Several factors push progression toward kidney failure. Risk rises with advancing age — especially above 60 years. Poorly controlled diabetes and chronic uncontrolled hypertension accelerate damage. Family history, smoking, obesity, and cardiovascular disease all contribute.
Some clinicians remember HOD-D: Hypertension, Obesity, Diabetes, and Drug and vascular damage. The practical lesson at CHPS compounds and district hospitals is early recognition of chronic kidney disease before kidneys reach end-stage. By then, urgent dialysis with a central line becomes the fallback when no mature fistula exists.
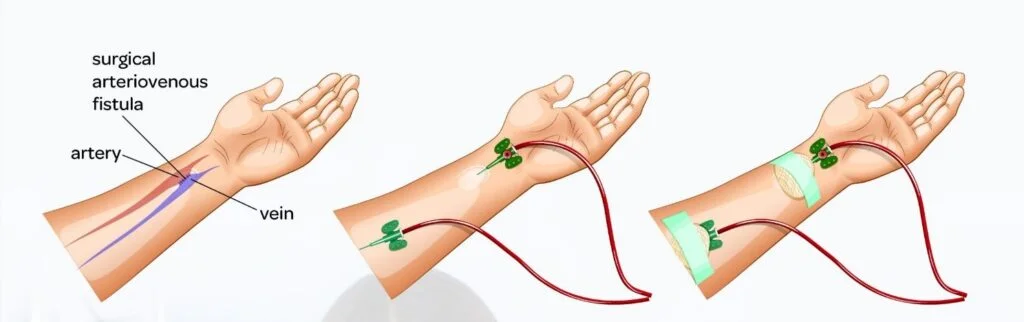
How a Fistula Forms: From Surgery to Needle-Ready Vein
Pathophysiology follows a clear sequence. A surgeon joins an artery directly to a vein. Arterial blood surges into the low-pressure vein. The vein gradually enlarges, thickens, and strengthens. Once mature, it tolerates repeated punctures and high flow. Hemodialysis becomes efficient. Think FLOW: Fistula created, Large blood flow, Outflow vein enlarges, Working dialysis access. Maturation typically takes six to twelve weeks. Signs include an enlarged vein, a palpable thrill, and an audible bruit. Fistulas should ideally be created before dialysis becomes urgent — not in the crisis of crashing kidney function when only a catheter will do.
Common surgical sites
Most fistulas are created in the upper limb:
- Radiocephalic fistula — the most common type; radial artery to cephalic vein, usually at the wrist
- Brachiocephalic fistula — brachial artery to cephalic vein, usually near the elbow
- Brachiobasilic fistula — brachial artery to basilic vein Site choice depends on vessel quality, anatomy, and surgical expertise available at your centre or referral hospital.
Signs of a Healthy Fistula — and Signs of Trouble
A functioning fistula announces itself. TAB captures the essentials: Thrill present, Audible bruit, Big visible vein. Warm skin over the fistula reflects increased blood flow. When things go wrong, symptoms vary:
Swelling — may indicate venous obstruction, infection, or thrombosis
Persistent pain — infection or ischemia
Weak thrill or absent bruit — clotting or blockage; loss of thrill especially suggests thrombosis
Bleeding — after needle removal or from ruptured aneurysm
Redness and fever — infection
Cold hand or fingers, numbness, tingling — possible steal syndrome, where blood is diverted away from the hand
Weakness or ulcers — also seen in steal syndrome
Patients and carers should feel for the thrill daily. A fistula that suddenly feels quiet is an
emergency, not a wait-and-see matter.
Complications: What Can Still Go Wrong
AV fistulas are the preferred access, but they are not complication-free. Remember SIT-BASH:
Stenosis — vessel narrowing reduces flow
Infection — less common than with catheters, but presents with redness, fever, pus
Thrombosis — among the commonest problems; caused by low flow or narrowing
Bleeding — from needle sites or ruptured aneurysms
Aneurysm — repeated needling weakens walls; bulging areas form
Steal syndrome — hand becomes cold, painful, weak; ulcers may develop
Heart failure — very large fistulas with high blood flow can strain the heart
Other problems include poor maturation (some fistulas never enlarge enough), venous hypertension causing arm swelling, and the psychological weight of a visible access site affecting body image, employment, and daily life. Supportive counselling helps many patients cope.
Diagnosis and Monitoring
Doctors monitor fistula function through clinical examination and targeted investigations.
Clinical examination assesses thrill, bruit, pulses, and swelling at every dialysis visit and during outpatient review.
Doppler ultrasound evaluates blood flow, vessel narrowing, and thrombosis — often the first imaging step when thrill weakens.
Fistulography uses contrast to identify blockages when intervention is planned.
Blood tests track kidney function, infection markers, and electrolytes in the broader dialysis care plan.
At centres without immediate vascular surgery, early ultrasound and referral to a unit that can
perform thrombectomy, angioplasty, or surgical revision may save a fistula that would otherwise be lost.
Management: Protecting the Lifeline
Management focuses on maintaining function and treating complications promptly.
Daily fistula care
Patients should keep the area clean, avoid trauma, and check the thrill every day.
Prevent compression: no tight clothing or jewellery on the fistula arm, no blood pressure measurements on that arm, and no sleeping on it. Needle rotation during cannulation reduces aneurysm formation. Good hygiene prevents infection.
Treating specific complications
Thrombosis may require thrombectomy, angioplasty, or surgical revision.
Infection needs antibiotics and drainage if an abscess forms.
Stenosis may respond to balloon angioplasty.
Severe aneurysm or poor function may need surgical revision.
Proper cannulation technique by trained dialysis nurses is part of prevention, not an afterthought.
Broader lifestyle measures
Good blood pressure control, diabetes management, healthy diet, and avoiding smoking all support both kidney health and vascular integrity. Well-maintained fistulas may last many years, though diabetes, vascular disease, smoking, and inconsistent care shorten survival.
Ghanaian Realities: Planning Before the Crisis
In practice, the gap between knowing fistulas are best and having one ready is where patients suffer. A farmer referred from a district hospital with newly diagnosed end-stage kidney disease may arrive at a teaching hospital needing immediate dialysis. Without a mature fistula, a central venous catheter becomes the bridge — higher infection risk, shorter lifespan, more emergency
visits. NHIS coverage for chronic dialysis and vascular surgery varies in implementation; families still navigate transport, lodging near urban centres, and lost income during treatment days.
The reframe for clinicians at every level: identify chronic kidney disease early, refer before crash, and plan fistula creation while creatinine is rising — not after the first emergency dialysis. Surgeons at regional and teaching hospitals can create fistulas electively. Medical officers can protect non-dominant arm veins from unnecessary cannulation and blood draws years before
dialysis is needed. Nurses at dialysis units can teach thrill-checking in Twi, Ga, or Ewe as readily as in English. Community health workers at CHPS can reinforce that swollen ankles plus uncontrolled diabetes or hypertension deserve investigation, not repeated diuretic prescriptions alone.
What Patients Should Know Before Going Home
If you or someone you love has a fistula or is approaching dialysis, carry these facts:
The thrill and bruit mean the fistula is working. Protect that arm like a lifeline — because it is one. Report swelling, pain, fever, bleeding, a cold hand, or a fistula that suddenly feels silent. Do not let anyone take blood pressure or draw blood from the fistula arm. Keep the site clean and avoid injury.
For clinicians, the summary is equally direct: AV fistulas are the preferred dialysis access. Thrill and bruit indicate proper function. Loss of thrill suggests thrombosis. Early creation and daily care improve survival and dialysis quality. With planning, education, and multidisciplinary follow-up across Ghana’s referral chain — from CHPS to district hospital to renal unit — many patients can keep a working fistula for years. That buzzing vein under the stethoscope is not a minor finding. It is the sound of time bought, access secured, and another dialysis session made possible.
Disclaimer
The information contained in this post is for general information purposes only. The information is provided by Everything You Need To Know About Arteriovenous Fistula In Renal Failure and while we endeavour to keep the information up to date and correct, we make no representations or warranties of any kind, express or implied, about the completeness, accuracy, reliability, suitability or availability with respect to the website or the information, products, services, or related graphics contained on the post for any purpose.